Introduction
Non communicable diseases (NCDs) kill 41 million people each year, equivalent to 71% of all deaths globally.1 Each year, more than 15 million people die from a NCD between the ages of 30 and 69 years; 85% of these "premature" deaths occur in low and middle-income countries.1 77% of all NCD deaths are in low- and middle-income countries.1 In India, Non-communicable diseases (NCDs) contribute to 60% of all deaths. The four major causes of NCD deaths are: Coronary Heart Disease, Stroke, and Hypertension (45%), Chronic respiratory disease (22%), Cancers (12 %), Diabetes (3%)2 One of the most serious concerns about Non-Communicable Diseases is that they affect people in the productive years of their life.2
Non-communicable diseases originate from unhealthy lifestyles and adverse physical and social environments. Well-known risk factors include poverty, poor diets like intake of foods rich in fat, salt and sugar; physical inactivity, consumption of tobacco, excessive use of alcohol and stress. The burden of Non-communicable diseases can be reduced through effective preventive measures. Physical inactivity, tobacco use, harmful use of alcohol are the behaviour risk factors that can be modified and should be targeted for NCD control.3, 4, 5, 6 Screening for NCD risk factors predicts the future risk of the disease in the population. Timely screening, diagnosis and prompt treatment of NCDs are key components to restrict the incidence of NCDs.7 Community Based Assessment Checklist (CBAC) score is one such simple screening tool that can be used to assess the risk of NCDs in communities viz. Hypertension, Diabetes and 3 common cancers Oral, breast and cervical cancer.2 Hence this study was undertaken in view to assess the risk of NCDs and in turn to serve as a tool for early diagnosis and treatment.
Materials and Methods
A cross-sectional study was carried out in month of January 2022 to May 2022 in Urban field practice area of IGGMC, Indora and rural field practice area of primary health care centre, Raipur at Nagpur district.
Ethical consideration
The study was approved by Institutional Ethics committee (IEC) of Indira Gandhi Government Medical College, Nagpur, Maharashtra, India. Written informed consent was be taken from participant before enrolling them in study; Confidentiality of the participant was assured and maintained throughout the study.
Exclusion criteria
Already diagnosed case of NCDs i.e Hypertension, Diabetes, Breast cancer, oral cancer and cervical cancer, severely ill patients and who refused to give consent were excluded from the study.
Sample size estimation
Where, n = sample size,
To calculate values for “p” study conducted by by Kaur MP et al.8 in Ambala district, Haryana, India, was used as reference for expected prevalence [57.7%] of adult population having risk of developing NCDs with CBAC score of > 4. Sample size derived was 376, however 188 study participants from rural area and 188 from urban area were included in the study.
Data collection
A predesigned pretested questionnaire was used to record socio-demographic data and Information about risk of NCDs using Community based assessment checklist2 (CBAC) namely Age, Tobacco consumption, Alcohol intake, Waist measurement, Physical inactivity, Family history and questions regarding 3 cancers viz, oral, breast and cervical cancer was recorded and score was given. Individual whose score was 4 and above along with those having any suggestive symptom of respective cancer were identified as having risk of developing NCDs. A preliminary test was conducted to ensure that the questions were clear and understandable. For data collection, house to house survey was done. Eligible respondent was selected from each of the households. Face to face interview technique was used and consecutive sampling method was adopted for selection of study participants till the sample size is achieved.The questionnaire consisted of two sections:
Section A) Socio-demographic characteristics details: Name, age, gender, educational level, place of residence, occupation, socio-economic status.
Section B) Community based assessment checklist which has two parts:
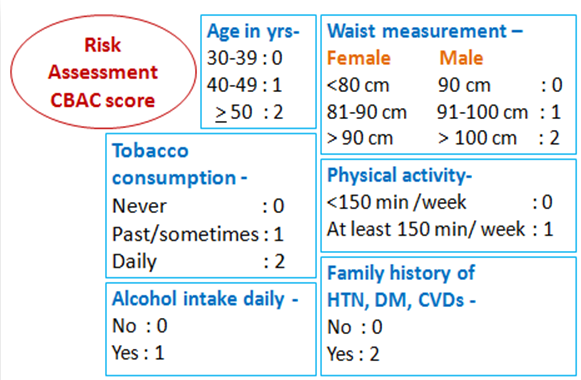
Table 1
Part B: Early detection symptoms for oral, breast and cervical cancer
After collecting the data, entry was done in MS EXCEL Version 2020. IBM Statistical Package for Social Sciences version 20 (SPSS V.20.0) software was used for analysis. Socio demographic data was organized and presented by applying principles of descriptive statistics. Chi-square is applied to find the association between the risk factors (alcohol use, physical inactivity, and waist circumference, smoking and family history) and CBAC score.
Results
Table 2
Socio-demographic characteristics of study participants as per residence
Table 2 Presents distribution of study participants according to socio-demographic characteristics. Out of 376 participants majority were female 51.1% and 48.9% were male. Maximum number of participants 123(32.7%) had completed education up to Intermediate or Diploma while 14(3.7%) were illiterate. Maximum 150(39.9%) belonged to socio economic class II.
Table 3
Distribution of study participants as per community based assessment checklist (CBAC) variables
[i] Overall mean age was 46.25 + 12.44 years , range : 50(30 - 80 ) years. Urban: M: 46.73 ± 12.62 years and range : 50 (30 – 80) years, F : 45.27 ± 12.04 years and range : 48 (30 – 78) years and Rural: M : 47.49 ± 12.13 years and range : 50 (30 – 80) years, F : 45.58 ± 13.01 years and range : 48 (30 – 78) years
[ii] Overall mean waist circumference 87.15 + 6.94 cms, range:32(72-104)cms . overall males : mean + SD = 91.13 + 5.03 cms,, range : 26 (78 – 104) cms , Overall females : mean + SD = 83.34 + 6.36 cms, range : 30(72 – 102) cms U: M: 92.13 + 4.75 cms, range : 22 (82 – 104) cms, F : 83.81 + 6.66 cms, range : 26 (72 – 98) cms and R: M : 90.16 + 5.13 cms, range : 24 (78 – 102) cms, F : 82.86 + 6.04 cms, range : 30 (72 – 102) cms
Table 3 Shows distribution of study participants as per Community based assessment checklist (CBAC) variables by residence. Most study participants 138(36.7%) belonged to age group 30-39. 54% of study population never used tobacco in lifetime. 99(26.3%) of respondents consumed in past or sometimes, out of these 12 were females whereas 74(19.7%) respondents were daily smokers , out of these 8 were females and all other 172 females were lifetime abstainers. Nearly 28(7.4%) of them were daily drinker all were male on the other hand all the female were lifetime abstainers. No significant difference found between place of residence and CBAC variables – age (p=0.599), tobacco use (p=0.147) and alcohol (0.556). Majority of the study participants from rural area 106(56.38%) had waist circumference 90 cm – 100cm while Least number of participants 8(4.26%) had waist circumference >100 cm. Maximum participants from urban area i.e. 95(50.53%) had waist circumference of 90cm -100cm while 20 (10.64%) had waist circumference >90 cm. Majority participants 299 (20.5 %) performed physical activity less than 150 minutes/week. 149(39.6%) of participants had family history of High Blood pressure, Diabetes and heart diseases while majority227(60.4%) had no family history of NCDs, the difference between CBAC variable viz. physical activity(p=0.201), family history of hypertension (p=0.206) and place of residence was not significant.

Figure 2 depicts that majority i.e 229 (60.9%) of study participants had risk of developing any NCDs with score ≥ 4 while 147(39.1%) of respondents had score less than 4. Mean score was 3.97 + 1.66 range 0 to 8.
Out of 376 study participants 5 were diagnosed to have ulcer in mouth for > 2 weeks as suspected symptom of oral cancer out of which three of them used tobacco daily and two used sometimes, no women had any suggestive symptoms of breast cancer while 3 had foul smelling vaginal discharge.
Table 4
Distribution of study participants based on community based assessment risk score as per residence.
|
Risk score |
Study participants |
x2 df p value |
|||||
|
Urban (n=188) |
Rural (n=188) |
Total n=(376) |
|||||
|
No |
% |
No |
% |
No |
% |
0.011 1 1 |
|
|
<4 |
74 |
39.4 |
73 |
38.8 |
147 |
39.1 |
|
|
≥ 4 |
114 |
60.6 |
115 |
61.2 |
229 |
60.9 |
|
Table 5
Association of NCD risk score with socio-demographic variables
Table 6
Association of NCD risk score with CBAC variables
Table 7
Association of NCD risk score with CBAC variables by residence
The risk of NCD with score ≥ 4 was found in 114(60.6%) of urban and 115(61.2%) of the rural participants, the difference between risk score and place of residence was not found to be significant (p = 1).
Table 5 Shows association of NCD risk score with socio-demographic variables. There was significant association found between NCD risk score and socio-demographic variables viz. gender (p=0.000) and education (p=0.042) while no significant association was found between NCD risk score and SES of the study participants.(p= 0.422).
Table 6 Shows most participants with score ≥ 4 belonged to age group 30-39 and the risk of NCD with score ≥ 4 was found to be significantly associated with CBAC variables viz. Age ( p=0.000), Tobacco consumption(p=0.000), Alcohol intake( p=0.000), Waist circumference (p= 0.000) and Family history of hypertension, Diabetes mellitus and cardiovascular illnesses ( p=0.000).
Table 7 Shows that among the participants with score ≥ 4 having risk of NCDs, there was no significant association found between place of residence and CBAC variable viz. age (p=0.837), Tobacco consumption (p=0.129), Alcohol intake( p=0.427), physical activity (p = 1) and Family history of hypertension, Diabetes mellitus and cardiovascular illnesses (p = 0.11) while the association was significant for Waist circumference (p= 0.03).
Discussion
Early detection of non-communicable diseases leads to better health outcomes. A cost-effective early risk detection strategy will act as the key in preventing the burden of NCDs. Community-Based Assessment Checklist (CBAC) is the population-based high-risk screening strategy for NCDs introduced in India at the primary health care level. The first validity study of a community-based assessment checklist as a comprehensive approach for assessing NCD risk in rural areas was conducted by Choudhary N et.al.9 Our study found the overall risk of common NCDs was 60.9% with cbac score ≥ 4 while 39.1% had score <4. The risk of common NCDs was 61.2% in rural area which was higher than in study by Kaur MP et.al.8 57.7% study participants had with cbac score ≥ 4 and nearly 42.3% of respondents had score less than 4. Kalidoss VK et.al. 10 observed that overall 70% had scored more than 4. Choudhary N et.al9 found that 28% individuals had CBAC score above 4, 48% at 4 and 24 % had a score below 4. In our study, 36.7% of study participants belonged to age group 30-39years and this finding was opposite to study conducted by Kaur MP et.al.8 where 41% of the respondents were more than equal to 50 years similar to findings of Kalidoss VK et.al10 and Choudhary N et.al9 where majority participants from age group above 50 years,71% and 64.66 % respectively. This may be because as most individuals > 50yrs from surveyed population of our study were already diagnosed case of NCDs hence were excluded from the study.
There were more females 192(51.1%) than males 184(48%) in our study in line with the study conducted by Kaur MP et.al.8 where 70.8% were females and in contrast to Kalidoss VK et.al.10 where 69% were male and Choudhary N et.al.9 found 145(64%) out of 266 males.
In the present study higher percent 203 (54%) of study participants never used tobacco were found, this may be due to majority participants were females 52% out of these 50 % females were lifetime abstainers and only 12(10.81%) females had past history of tobacco use whereas 8(8.08%) of female respondents had daily tobacco use this finding was similar with Choudhary N et.al.9 where tobacco consumption was 10.5% and less than that found in the study conducted by Kalidoss VK et.al.10 where 12% of participants used tobacco daily while tobacco use was found higher in study by Maimela E et.al.11 81.3% and the second global tobacco adult survey which showed 20% current tobacco.12
Nearly 28(7.4%) of the male respondents were daily drinker higher than found in Kalidoss VK et.al.10 study where 6% using alcohol daily and lower than found in Choudhary N et.al.9 study i.e. 11.27% and Krishnan A et.al.13 as 24.6% among men while women were abstainer this is consistent with our study where all the female were lifetime abstainers.
Waist circumference of more than 100cm in men and >90cm in female which is considered high risk was 7.45% in our study which was lower as observed in Choudhary N et.al.9 36%. Overall 229(79.5%) of study participants performed physical activity less than 150 minutes/week was more than that as observed by Kaur MP et.al.8 where it was 71.4% and Kalidoss VK et.al.10 where 60% did not have adequate physical activity. Choudhary N et.al.9 study reported 52% had physical inactivity similar findings were observed by Nelson F et.al.14 and Sandhu S et.al.15 with physical inactivity in 54.3% and 51% study participants respectively.
Our study found 149 (39.6%) of participants had family history of High Blood pressure, Diabetes and cardiovascular diseases much less than reported by Kaur MP et.al.8 Kalidoss VK et.al.10 and Choudhary N et.al 9 where family history was found in 42.9%, 48.2 % and 49.24% in respectively.
In present study significant relationship was seen between age and risk of NCD (p = 0.000) and this finding was supported by the study conducted in Kathmandu, Nepal by Dhungana RR et al (2014).16 and were also alike with the results of a study conducted by Bansal P et al (2016).1 The risk of NCD was found to be significantly associated with CBAC variables viz. tobacco use (p= 0.000), alcohol consumption (p = 0.000), waist circumference (p = 0.000), and family history of hypertension, Diabetes mellitus and cardiovascular illnesses (p=0.000) were found have significant association with the risk of developing NCD these findings are in line with similar study conducted by Kaur MP et.al.8 except for tobacco use. A cross-sectional study conducted by Premanandh K et.al.17 also showed that abdominal obesity and alcohol consumption were significantly associated with higher CVD risk.
In our study, there was no significant association seen been NCD risk and CBAC variable by place of residence. There is lack of data from studies which included both rural and urban population simultaneously. In our study Only 5 study participants were diagnosed to have ulcer in mouth out of which three of them used tobacco daily and two used sometimes, no women had any suggestive symptoms of breast cancer while three had foul smelling vaginal discharge. These suspected symptoms were not considered in the previous studies conducted for assessing risk factors of NCDs using CBAC.
Conclusion and Recommendations
Overall risk of NCD was found to be 60.9% in adults of urban and rural field practice area of IGGMC, Nagpur. Majority of the CBAC variables were found to have significant association with increase NCDs risk. CBAC is a very simple easy to employ tool that can be used to screen communities for identifying people at risk of NCDs. This may further help to plan and implement strategies and assist early intervention among the recognized high risk population which in turn will further restrict the burden of NCDs.
Limitation
The study is an observational study and did not involve any investigation for further screening of participants with high risk score for NCDs. Risk factors like family history may not be known to all the participants and alcohol consumption, tobacco consumption, physical activity may not be reported correctly by participants.