- Visibility 0.9k Views
- Downloads 137 Downloads
- Permissions
- DOI 10.18231/j.jchm.2024.036
-
CrossMark

Evaluating the effects of hands-only CPR training on knowledge, attitudes, and altruistic behavior among school children in rural India
- Author Details:
-
 Sachita Pari Tiwari *
Sachita Pari Tiwari *
-
Neelam Anupama Toppo
-
Sai P Tiwari
Abstract
Background: A significant increase in sudden heart attacks among Indian men under 50 years old has been observed nationwide. Survival from cardiac arrest largely depends on how quickly CPR is started and the quality of CPR given. People who receive effective bystander CPR are 2-3 times more likely to survive, but many people lack the knowledge to recognize or respond to a cardiac arrest emergency especially in rural India. This research examines the effectiveness of Hands-Only CPR training in enhancing schoolchildren's knowledge, attitudes, and responses in rural India.
Aims & Objectives: To investigate effects of Hands-Only CPR training on CPR knowledge in school girls, investigate effects of Hands-Only CPR training on the willingness, attitudes, & intentions toward helping others and performing CPR and assess the potential of targeted educational interventions at schools, to improve community response in cardiac emergencies and improving survival rates.
Materials and Methods: Setting- girls’ High school in Barela, a rural town with limited resources in the Jabalpur District. The Cross-sectional Pre and Post intervention study took place at P.M. SHRI Government Higher Secondary School for Girls in Barela, Jabalpur, Madhya Pradesh, a rural town with limited resources in the Jabalpur District. Study Design- The Cross-sectional Pre and Post intervention study to obtain quantitative data on the effectiveness of the educational intervention of Hands Only CPR. Pre-training and post-training assessments were used to measure changes in the participants' knowledge, attitudes, and willingness to perform CPR.
Results: None of the participants knew what CPR or Basic Life Support prior to the training. Significant improvement was noted on knowledge towards recognizing signs of life, steps of Hands only CPR amongst the participants. Comfort on performing CPR and willingness to help during cardiac emergencies after the CPR training significantly improved
Conclusion: Our study identifies a notable gap in the awareness and preparedness of the students, highlighting the need for comprehensive CPR training programs at a high school level in rural India, to improve public health outcomes. Our study suggest that targeted educational interventions could empower communities and reduce the impact of cardiac emergencies.
Introduction
According to the study report “India: Health of the Nation’s States”. The India State-Level Disease Burden Initiative in 2017, conducted by the Indian Council of Medical Research (ICMR), it is estimated that the proportion of deaths due to Non-Communicable Diseases (NCDs) in India has increased from 37.9% in 1990 to 61.8% in 2016. Most of them are cardiovascular deaths. As per a 2012 study[1] approximately 10.3% or 700,000 Sudden Cardiac Death (SCD) cases occurred in India annually, with 21% affecting individuals under the age of 50. The number of deaths due to sudden cardiac death (SCD) has significantly increased in India over more than a decade, grabbing a lot of public and media attention and emphasizing the urgent need for community CPR education to save lives. India, along with other developing countries, is experiencing a rise in cardiovascular disease driven by changing lifestyles, a concern also highlighted by The Lancet Commission on SCD.[2]
Survival rates from sudden cardiac arrest (SCA) remain below 10% in most parts of the world.[3] The Lancet Commission emphasizes the importance of community involvement in responding to SCA, including bystander Cardiopulmonary Resuscitation (CPR) and public access to automated external defibrillators (AEDs), to improve survival rates.[2] Research indicates that immediate CPR and AED use can increase survival rates from less than 10% to around 70%. Early recognition and intervention are crucial in preventing death and disability, but many people lack the knowledge to recognize or respond to a cardiac arrest emergency. Survival from cardiac arrest largely depends on how quickly CPR is started and the quality of CPR given. People who receive effective bystander CPR are 2-3 times more likely to survive. Hands-Only CPR during a cardiac emergency is critical to begin the chain of survival. Out-of-hospital cardiac arrest (OHCA) is a public health burden accounting for nearly 10% of global mortality and 50% of cardiovascular deaths.[4] In India, over 92% of sudden cardiac arrests happen outside of hospitals, most commonly in residential settings.[3] About 90% of patients who are victims of out-of-hospital cardiac arrest (OHCA) die before reaching the hospital; this emphasizes that Cardiopulmonary resuscitation (CPR) is the most critical step in the survival link chain of OHCA, and it is imperative to recognize symptoms and signs of sudden cardiac arrest (SCA) to ensure timely intervention.[5], [6] Given that most OHCAs occur at home[3] bystanders are required to provide BLS until the arrival of emergency medical services.
Despite these statistics, CPR training is not integrated into the school curriculum, exacerbating the challenge of low bystander CPR rates in India, reported between 1.3% and 9.8%.[3], [7] This is well below the target goal of 62% set by the American Heart Association Emergency Cardiovascular Care (AHA-ECC) for effective bystander CPR rates.[8] With an estimated survival of less than 10%, OHCA remains one of India's leading causes of death.[3], [5] In addition, education and awareness regarding the identification of SCA remains low, contributing to poor bystander CPR rates.[9], [10] Poor knowledge of cardiopulmonary resuscitation (CPR)[11] and inadequate provision of bystander CPR due to cultural factors such as gender, race, and class differences also exist in society due to fear of being judged. Inadequate knowledge and skill of understanding what an OHCA event is, the critical role of survival link associated with resuscitative measures, along with lack of training in performing CPR continue to exist. [12]
Awareness of the importance of CPR must be raised in early childhood education, [13] as CPR training improves the safety culture in schools and shifts the responsibility from adults to children, which could result in long-term structural changes. [14] The introduction of CPR training in schools has been advocated by the World Health Organization. [15]
In Scandinavia, teaching school children CPR has increased lay bystander CPR rates, resulting in higher survival rates after OHCA and lowering healthcare costs. [16] Teaching the importance of OHCA recognition and CPR skills should begin early, as schoolchildren are more motivated, learn faster than adults, and retain their skills better. [17], [18]
In some countries, CPR training for schoolchildren is already mandatory, while in others it is being gradually introduced into curriculum. [15] If learned CPR at a young age, Children are likely to retain these lifesaving skills, much like swimming or bike-riding skills[19] and can serve as CPR multipliers by passing on the acquired awareness and CPR skills to family members and friends. [20] The advantages of early CPR teaching include a positive attitude toward helping others, increased confidence in the success of resuscitation, internal motivation to assist those in need, and the development of empathy. [21], [22]
Behavioral changes ([Figure 3]) can be more effective when supported by appropriate structural measures, such as education and awareness-raising, particularly in the field of public health.[22] Panchal et al., [23] claim that interventions aimed at changing behavior are most effective when grounded in theory. Both the Social Learning Theory and the Theory of Planned Behavior were developed to enhance health education and ensure behavior change. [24] Based on the theoretical grounding and the presentation of the Intention-Focused Model of Bystander CPR by Panchal et al., [23] it is anticipated that early CPR training will influence individuals' willingness, attitudes, and intentions toward assisting others and performing CPR. According to the model, changes in intention are likely to lead to changes in behavior when individuals possess the skills and ability to act. Panchal et al. predict that such changes in intention will lead to behavior changes, potentially resulting in improved CPR outcomes. [25] The Intention-Focused Model by Panchal et al. is grounded in well-validated theories, including Ajzen’s Theory of Planned Behavior. [26] According to Ajzen, “intentions are assumed to capture the motivational factors that influence a behavior; they are indications of how hard people are willing to try, of how much of an effort they are planning to exert, in order to perform the behavior”. [26] Based on these two theories, and as demonstrated by Pivač et al., [22] our study expects to see improvement on Knowledge, Attitudes, and change in Altruistic Behavior Among Schoolchildren after providing Hands-Only CPR training.
Aim and Objective of the Study
Investigate effects of Hands-Only CPR training on CPR knowledge in school girls.
Investigate effects of Hands-Only CPR training on the willingness, attitudes, and intentions toward helping others and performing CPR.
By focusing on this demographic, we sought to assess the potential of targeted educational interventions to improve community response to cardiac emergencies and ultimately enhance survival rates.
Material and Methods
Setting
The Cross-sectional Pre and Post intervention study took place at P.M. SHRI Government Higher Secondary School for Girls in Barela, Jabalpur, Madhya Pradesh, a rural town with limited resources in the Jabalpur District.
Study design
A quantitative research design was employed for this study. Specifically, a separate pre-post intervention study design was conducted to obtain quantitative data on the effectiveness of the educational intervention training of Hands Only CPR training was implemented. [14], [15], [22] Pre-training and post-training assessments were used to measure changes in the participants' knowledge, attitudes, and willingness to perform CPR.
Participants
Inclusion Criteria was female students from grades 8 to 12. 200 students received Hands only CPR training, out of which 102 students, voluntarily participated in both pre- and post-training surveys. No significant differences were established in the sample structure prior to and after CPR training according to age distribution, which means that both samples were uniform. Distribution of schoolchildren was equal prior to and after training
Study tools and techniques
Survey questions
Participants completed a structured questionnaire consisting of two sections with 18 nominal-level binary questions. The questionnaire was designed by Authors in Hindi to accommodate the Hindi-medium school setting.
Section 1: Knowledge Assessment
The first section included 9 knowledge-based questions designed to evaluate participants' understanding of CPR procedures and emergency response protocols. Questions included assessing scene safety, recognizing signs of life, steps of CPR, Site and duration of pulse check during CPR, Recommended site, rate and Depth of Chest compressions and chest to Breath compression Ratio during CPR.
Section 2: Altruistic Behavior
The second section comprised 9 statements assessing participants' attitudes and willingness toward performing CPR in emergencies. Participants responded using a nominal-level scale (Yes/No/Maybe) to statements reflecting their confidence in identifying signs of life, confidence in providing assistance and their understanding of CPR's life-saving potential.
Procedure
At the beginning of each session, participants were given a pre-survey and allotted 10 minutes to complete it. They were assured that their responses would not affect their grades and were encouraged to provide honest answers without assistance. In the survey, the girls were also inquired about their age, grade, and number of adults in their family (to estimate how many people would be impacted by their knowledge of administering CPR). Following the pre-survey, all participants received instruction in Hindi on the steps required to respond to an unresponsive victim. This included information on scene safety assessment, ACT (Assess, Call for Help, Treatment) protocol, and CPR techniques such as correct speed, depth, and hand placement during chest compressions. Hands-on training followed, focusing on the proper administration of Hands-Only CPR using a manikin. This practical session allowed participants to apply the knowledge gained from the theoretical instruction. Subsequently, all participants completed the same self-administered questionnaire to assess changes in attitudes, willingness, and knowledge related to CPR after the training session.
For research purposes, the instructor delivered consistent educational content using uniform teaching methods aligned with the national Hands-Only CPR program. This program draws from guidelines established by the American Heart Association (AHA) and AIIMS, designed to train students, community healthcare workers, and the public in effective CPR techniques.
Data analysis
Answers to binary questions were converted to numerical data to improve prediction accuracy. We calculated the percentage improvement for each knowledge-related question with CPR training. Paired t-tests were performed, and p-values were calculated to determine if there were significant differences between pre- and post-training responses. Mean and standard deviation calculations, paired t-tests, and p-value determination was applied to assess the statistical significance of changes in altruistic behavior pre- and post-training.
Results
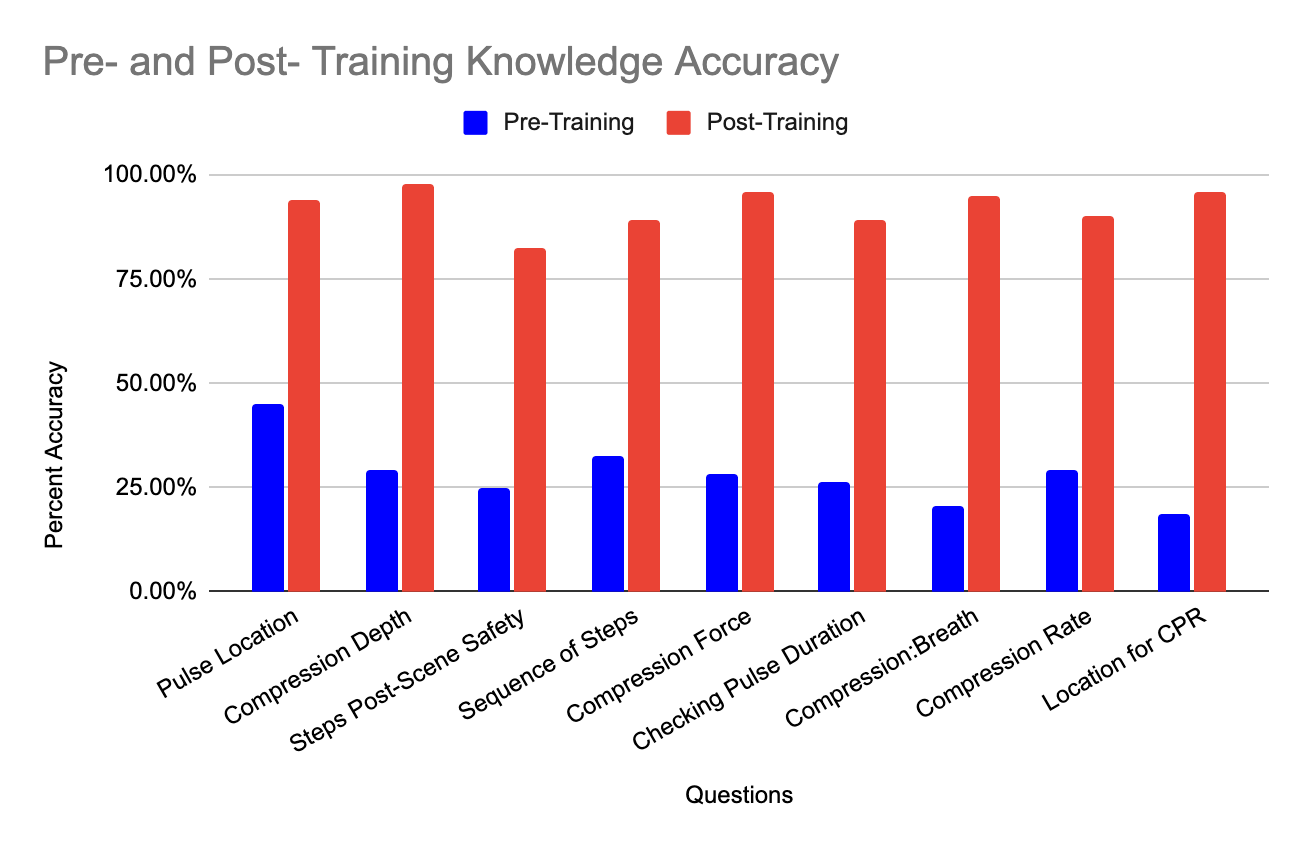
As shown in [Table 1], participants had limited knowledge of CPR prior to the training session. However, after receiving hands-on CPR training, a statistically significant improvement was observed in several key components of CPR, including the ability to locate the pulse on victims, the correct depth of chest compressions, assessing a victim’s responsiveness, following the correct sequence of CPR steps, performing high-quality chest compressions, determining the appropriate duration for carotid pulse checking, understanding the compression-to-breath ratio, the correct chest compression rate, and identifying the proper location for chest compressions ([Figure 1]). These skills are critical for improving the survival rates of cardiac arrest victims.
The results of the altruistic behavior questions ([Table 2]) are as follows
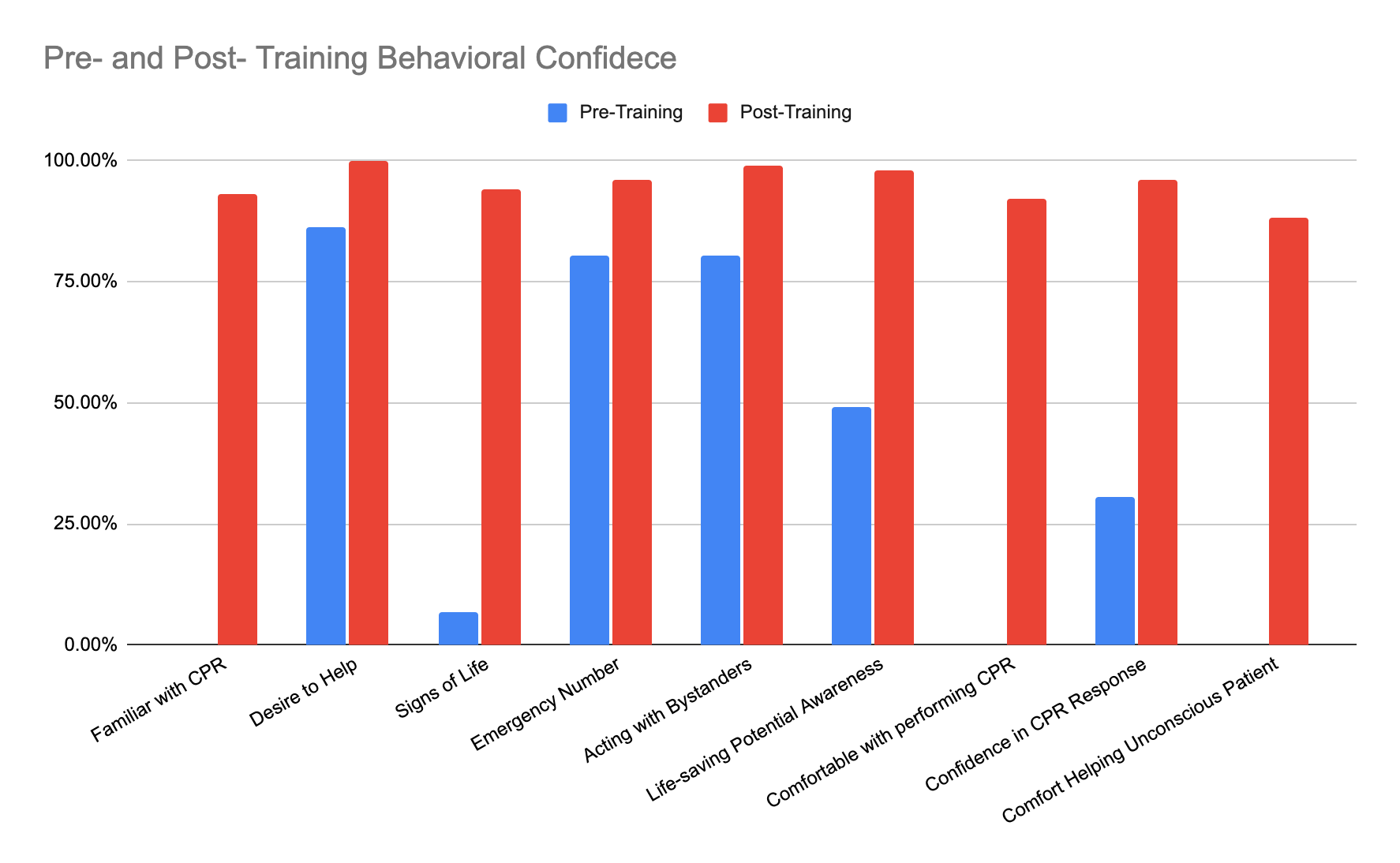
Before the training, none of the participants knew what CPR or Basic Life Support (BLS) was. After the training, over 93% of participants understood the concept of CPR. Initially, more than 86% of participants were willing to assist someone who had fallen, over 80% knew India’s universal emergency ambulance number, and more than 80% were willing to provide CPR instead of remaining bystanders during a sudden cardiac arrest (SCA) emergency. Post-training, a statistically significant improvement was noted in participants' attitudes toward helping others. Fewer than 7% of participants knew how to identify signs of life prior to the training. This figure increased to 94% post-training (p-value < 0.005).
Initially, fewer than half of the participants were aware of the life-saving potential of CPR. After the training, over 98% recognized its importance, reflecting a statistically significant improvement. None of the participants felt comfortable initiating CPR before the training. Following the training, 92% expressed confidence in performing CPR. Before the training, only one-third of participants believed they could initiate Basic Life Support to save a life. This confidence rose to over 96% after the training. Comfort in providing Basic Life Support to an unconscious person increased from 0% before training to 88% afterward ([Figure 2], [Figure 3]).
|
Knowledge assessed |
Correctly answered before training |
Correctly answered after training |
t-statistics |
p-value |
|
Correct Pulse location |
45% |
94% |
-8.567521 |
<0.005 |
|
Chest Compression depth |
30% |
98% |
-14.709304 |
<0.005 |
|
Step after scene safety |
25% |
82% |
-10.51064 |
<0.005 |
|
Sequences of CPR steps |
33% |
89% |
-11.465891 |
<0.005 |
|
Chest Compression method |
28% |
96% |
-14.094277 |
<0.005 |
|
Time needed to check pulse |
27% |
89% |
-12.434759 |
<0.005 |
|
Chest Compression to rescue Breath Ratio |
20% |
95% |
-16.549744 |
<0.005 |
|
Rate of chest compressions |
29% |
90% |
-11.358322 |
<0.005 |
|
Correct location for chest compression |
19% |
96% |
-18.323482 |
<0.005 |
|
Behavior Measured |
Pre-Training Mean |
Post-Training Mean |
p-value |
Significant |
|
Familiarity with CPR |
0.107843 |
0.955882 |
<0.005 |
True |
|
Desire to Help |
0.887255 |
1 |
<0.005 |
True |
|
How to check signs of life |
0.171569 |
0.960784 |
<0.005 |
True |
|
Emergency number information |
0.818627 |
0.970588 |
<0.005 |
True |
|
Coming forward to help victim in public |
0.813725 |
0.995098 |
<0.005 |
True |
|
Lifesaving potential awareness |
0.563725 |
0.985294 |
<0.005 |
True |
|
Comfortable in providing CPR |
0.107843 |
0.955882 |
<0.005 |
True |
|
Confidence in providing CPR |
0.421569 |
0.980392 |
<0.005 |
True |
|
Comfortable in providing basic life support |
0.083333 |
0.931373 |
<0.005 |
True |

Discussion
Our study found significant improvements in both knowledge and altruistic behavior regarding Hands-Only CPR among schoolchildren in rural India following the training program. Notably, the percentage of girls who knew what CPR was increased from 0.00% to 93.14%, underscoring the effectiveness of the intervention. Similarly, other researchers found not only greater knowledge after CPR training, but also its retention. [22], [27], [28] Confidence levels and willingness to help others rather than being passive bystanders also saw significant gains. Similar conclusions were also reached by previous researchers. [22], [27], [29] Similar to a previous systemic review, [30] The participants exhibited substantial improvement in their knowledge of various CPR aspects, including the correct location, depth, speed of chest compressions, and other procedural steps.
Despite these positive outcomes, the study had some limitations. The sample was restricted to female students from a single rural school due to being girls only school. The short-term nature of the study does not address long-term retention of CPR skills and knowledge. Future research should investigate long-term retention and include a more diverse demographic to generalize the findings. Exploring the incorporation of AED training and addressing barriers to performing CPR could further enhance program effectiveness. [31], [32]
Initially, none of the students reported any knowledge of CPR, a fact corroborated by their teachers, who also lacked CPR training. While the students were familiar with the emergency ambulance number for India, they lacked other crucial CPR-related information. An additional option of "I don't know" for survey questions could have yielded more accurate pre-training data, as the current format might have led to random guessing. This could have better highlighted the knowledge improvement post-training.
With CPR knowledge, these girls are better equipped to assist in emergencies, potentially saving lives within their families and communities. This emphasizes the urgent need to integrate CPR training into Indian school curriculums. Educating young individuals about CPR can empower them to act during cardiac emergencies, potentially improving survival rates from out-of-hospital cardiac arrests. Such initiatives could profoundly impact public health, particularly in rural areas where medical resources are limited.
Conclusion
Our study identifies a notable gap in the awareness and preparedness of the students, highlighting the need for comprehensive CPR training programs at a high school level in rural India, to improve public health outcomes. The study demonstrates that school-based Hands-Only CPR training programs can significantly enhance schoolchildren's knowledge and attitudes toward cardiac emergencies. These targeted educational interventions could empower communities and reduce the impact of cardiac emergencies by reducing fatalities and long-term disabilities.
Such educational interventions have been successfully implemented in many developed countries in the west and are essential in bridging the gap in awareness and preparedness on sudden cardiac emergencies, ultimately contributing to increased chances of survival after cardiac arrest. This could be a vital step in creating a community capable of responding effectively to cardiac emergencies. Training school children in cardiopulmonary resuscitation worldwide is now endorsed by the World Health Organization (WHO). [15]
Conflict of Interest
None.
Source of Funding
None.
Acknowledgements
References
- Rao B, Sastry B, Chugh S, Kalavakolanu S, Christopher J, Shangula D. Contribution of sudden cardiac death to total mortality in India - a population based study. Int J Cardiol. 2012;154(2):163-7. [Google Scholar]
- Marijon E, Narayanan K, Smith K, Barra S, Basso C, Blom M. The Lancet Commission to reduce the global burden of sudden cardiac death: A call for multidisciplinary action. Lancet. 2023;402(23):883-936. [Google Scholar]
- Krishna C, Showkat H, Taktani M, Khatri V. Out of hospital cardiac arrest resuscitation outcome in North India - CARO study. World J Emerg Med. 2017;8(3):200-5. [Google Scholar]
- Berdowski J, Berg R, Tijssen J, Koster R. Global incidences of out-of-hospital cardiac arrest and survival rates: systematic review of 67 prospective studies. Resuscitation. 2010;81(11):1479-87. [Google Scholar]
- Yan S, Gan Y, Jiang N, Wang R, Chen Y, Luo Z. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Crit Care. 2020;24(1). [Google Scholar] [Crossref]
- Ritter G, Wolfe R, Goldstein S, Landis J, Vasu C, Acheson A. The effect of bystander CPR on survival of out-of-hospital cardiac arrest victims. Am Heart J. 1985;110(5):932-7. [Google Scholar]
- Adielsson A, Hollenberg J, Karlsson T, Lindqvist J, Lundin S, Silfverstolpe J. Increase in survival and bystander CPR in out-of-hospital shockable arrhythmia: bystander CPR and female gender are predictors of improved outcome. Experiences from Sweden in an 18-year perspective. Heart. 2011;97(17):1391-6. [Google Scholar]
- Kiguchi T, Okubo M, Nishiyama C, Maconochie I, Ong M, Kern K. Out-of-hospital cardiac arrest across the World: First report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation. 2020;152:39-49. [Google Scholar] [Crossref]
- Bhat R, Ravindra P, Sahu AK, Mathew R, Wilson W. Study of pre-hospital care of out of hospital cardiac arrest victims and their outcome in a tertiary care hospital in India. Indian Heart J. 2021;73(4):446-50. [Google Scholar]
- Kronick S, Kurz M, Lin S, Edelson D, Berg R, Billi J. Part 4: Systems of Care and Continuous Quality Improvement: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132(18 Suppl 2):397-13. [Google Scholar]
- Aroor A, Saya R, Attar N, Saya G, Ravinanthanan M. Awareness about basic life support and emergency medical services and its associated factors among students in a tertiary care hospital in South India. J Emerg Trauma Shock. 2014;7(3):166-9. [Google Scholar]
- Joseph N, Narayanan T, Zakaria SB, Nair A, Belayutham L, Subramanian A. Awareness, attitudes and practices of first aid among school teachers in Mangalore, south India. J Prim Health Care. 2015;7(4):274-81. [Google Scholar]
- Rensburg LCV, Richmond L, Mgidi S, Claassen J, Wylie C, Stassen W. The lay descriptors of out-of-hospital cardiac arrest in the Western Cape province, South Africa. Resusc Plus. 2021;7. [Google Scholar] [Crossref]
- Duber H, Mcnellan C, Wollum A, Phillips B, Allen K, Brown J. Public knowledge of cardiovascular disease and response to acute cardiac events in three cities in China and India. Heart. 2018;104(1):67-72. [Google Scholar]
- Buck ED, Laermans J, Vanhove A. An educational pathway and teaching materials for first aid training of children in sub-Saharan Africa based on the best available evidence. BMC Public Health. 2020;20. [Google Scholar] [Crossref]
- Calicchia S, Cangiano G, Capanna S, Rosa M, Papaleo B. Teaching life-saving manoeuvres in primary school. Biomed Res Int. 2016. [Google Scholar] [Crossref]
- Böttiger B, Aken H. Kids save lives--Training school children in cardiopulmonary resuscitation worldwide is now endorsed by the World Health Organization (WHO). Resuscitation. 2015;94:5-7. [Google Scholar] [Crossref]
- Wissenberg M, Lippert F, Folke F, Weeke P, Hansen C, Christensen E. Association of national initiatives to improve cardiac arrest management with rates of bystander intervention and patient survival after out-of-hospital cardiac arrest. JAMA. 2013;310(13):1377-84. [Google Scholar]
- Markenson D, Ferguson J, Chameides L, Cassan P, Chung K, Epstein J. Part 17: first aid: 2010 American Heart Association and American Red Cross Guidelines for First Aid. Circulation. 2010;122(18 Suppl 3):934-46. [Google Scholar]
- Banfai B, Pek E, Pandur A, Csonka H, Betlehem J. The year of first aid’: effectiveness of a 3-day first aid programme for 7-14-year-old primary schoolchildren. Emerg Med J. 2017;34(8):526-32. [Google Scholar]
- Buck E, Remoortel H, Dieltjens T, Verstraeten H, Clarysse M, Moens O. Evidence-based educational pathway for the integration of first aid training in school curricula. Resuscitation. 2015;94:8-22. [Google Scholar] [Crossref]
- Greif R, Lockey A, Conaghan P, Lippert A, Vries W, Monsieurs K. European resuscitation council guidelines for resuscitation 2015. Section 10. Education and implementation of resuscitation. Resuscitation. 2015;95:288-301. [Google Scholar] [Crossref]
- Pivačc S, Gradišek P, Skela-Savič B. The impact of cardiopulmonary resuscitation (CPR) training on schoolchildren and their CPR knowledge, attitudes toward CPR, and willingness to help others and to perform CPR: mixed methods research design. BMC Public Health. 2020;20(1). [Google Scholar] [Crossref]
- Laverack G. The challenge of behavior change and health promotion. Challenges. 2017;8(2). [Google Scholar] [Crossref]
- Decety J, Bartal I, Uzefovsky F, Knafo-Noam A. Empathy as a driver of prosocial behaviour: highly conserved neurobehavioural mechanisms across species. Philos Trans R Soc Lond B Biol Sci. 2016;371. [Google Scholar] [Crossref]
- Panchal A, Fishman J, Camp-Rogers T, Starodub R, Merchant R. An "Intention-Focused" paradigm for improving bystander CPR performance. Resuscitation. 2015;88:48-51. [Google Scholar] [Crossref]
- Reed M, Lloyd B. . Health psychology. 2018. [Google Scholar]
- Ajzen I. The theory of planned behavior. Organizational Behav Human Decis Processes. 1991;50(2):179-11. [Google Scholar]
- Naqvi S, Siddiqi R, Hussain SA, Batool H, Arshad H. School children training for basic life support. J Coll Physicians Surg Pak. 2011;21(10):611-5. [Google Scholar]
- Lukas R, Aken HV, Mölhoff T, Weber T, Rammert M, Wild E. Kids save lives: a six-year longitudinal study of schoolchildren learning cardiopulmonary resuscitation: Who should do the teaching and will the effects last?. Resuscitation. 2016;101:35-40. [Google Scholar] [Crossref]
- Maconochie I, Bingham B, Simpson S. Teaching children basic life support skills. BMJ. 2007;334(7605). [Google Scholar] [Crossref]
- Nombulelo E, Zenani. Bashir Bello,2 Matsipane Molekodi,1 and Ushotanefe Useh2. Effectiveness of school-based CPR training among adolescents to enhance knowledge and skills in CPR: A systematic review. Curationis. 2022;45(1):e1-9. [Google Scholar] [Crossref]